Key takeaways
- Patient acquisition is one system with three parts: owned, earned, and paid.
- Fund your website, profile, reviews, and booking before any ads.
- Aesthetics patients buy on trust, so the funnel runs slower.
- Track cost per booked patient, not leads. No universal benchmark exists.
Every guide hands you the same menu. Website, SEO, Google Business Profile, ads, reviews, referrals, online booking. All of it is useful. None of it tells you the one thing you actually need to know: which patient acquisition strategies to fund first, for a clinic at your stage, on your budget. That is the gap this page fills. The best moves aren't a checklist you switch on all at once. They're a sequence you fund in order, built around how cash-pay aesthetics patients really decide.
What patient acquisition means, and why it isn't retention
Patient acquisition is the work of attracting someone new and guiding them from first interest to a booked, completed visit. The goal is not a form fill or a follow. It is a person in your chair who showed up and paid.
Here is the part most menus skip. Winning a new patient costs a lot more than keeping one you already have. So acquisition spend only earns its place once your retention is solid. If patients book once and never come back, more ads just pour money into a leaky bucket. Fix the bucket first. Then fund the funnel.
Why acquiring an aesthetics patient is a different job
An aesthetics patient is not booking a same-day strep test. They are weighing an elective procedure that involves needles or lasers, changes how they look, and costs anywhere from a few hundred to several thousand dollars. It is not returnable. That makes it a high-consideration, emotional decision, and it changes what your funnel has to do.
A general clinic can capture a lead and convert it fast. You can't. Your prospect needs proof and reassurance before they commit. Real before-and-after results. A consult that answers their fears. Reviews from people like them. This trust-building lengthens the funnel, so it runs slower and leans on the consult. Channels tuned for instant, low-stakes bookings will quietly underperform here.
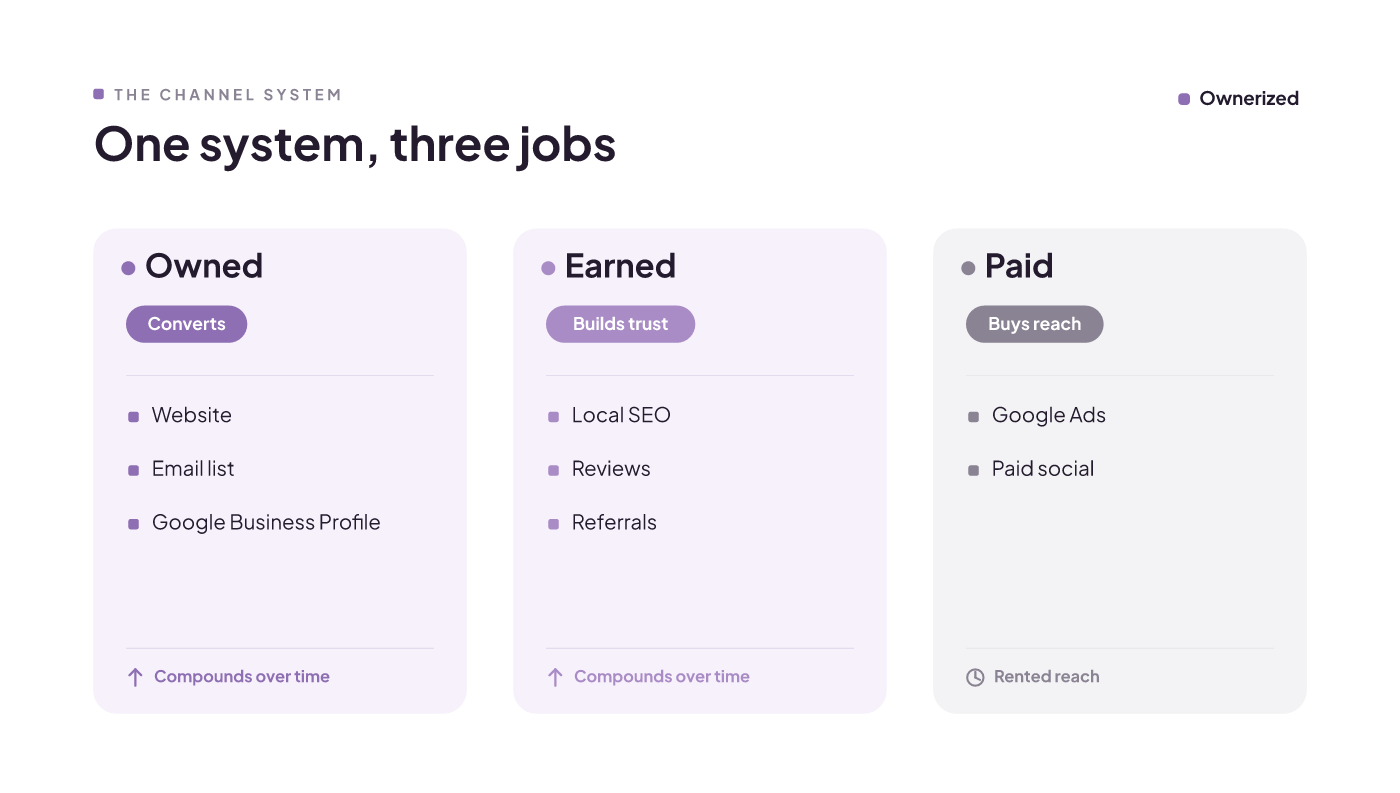
Owned, earned, and paid: what each channel is actually for
Sort every tactic into three buckets, because each does a different job.
Owned is what you control: your website, your email list, your Google Business Profile. This is where conversion happens. Your website is the front door of your clinic online, and a slow or dated site loses people before they ever reach out. A sharp site plus a complete Google Business Profile turns a searcher into a booked patient.
Earned is the trust you build over time: local SEO, patient reviews, and referrals. Prospective patients lean on reviews before they book, so your reputation does real selling for you. Earned channels are slow to build and hard for a rival to copy.
Paid is the reach you rent: Google Ads and paid social. Google still handles the overwhelming majority of searches, so paid search puts you in front of people already looking. The catch is simple. Paid attention stops the moment you stop paying. Owned and earned compound; paid does not. A clinic that leans only on Ads owns nothing when the budget pauses.
Which channels to fund first, by clinic stage and budget
This is the part every ranking guide skips. The logic underneath the grid is the owned, earned, and paid split from the last section: your website and Google Business Profile convert, reviews and referrals build trust, and paid buys reach. So a tactic that wastes money for a brand-new clinic can be the right first spend for an established one. Here is the same set of channels, mapped to where you are and what you can spend. Read the cell, not the row.
| Channel | Brand-new clinic (tight budget) | Established clinic (steady budget) | Multi-location (larger budget) |
|---|---|---|---|
| Website + Google Business Profile + local SEO | Fund now. It's the front door. Skip it and every other dollar leaks. | Fund now. Keep it fast and current. | Fund now. One strong profile per site, plus location pages. |
| Reviews and reputation | Fund now. Ask from day one. It costs little and compounds. | Fund now. Make the ask systematic after each visit. | Fund now. Watch review quality per location. |
| Online booking | Fund now. Removes the phone-call barrier that drops bookings. | Fund now. Connect it to your calendar and records. | Fund now. Standardize the flow across sites. |
| Referrals and word-of-mouth | Later. You need a happy patient base first. | Fund now. Ask satisfied patients on purpose. | Fund now. Build a repeatable referral offer. |
| Google Ads (paid search) | Later. Wait until the site and profile actually convert. | Fund now. Target high-intent local searches. | Fund now. Split budget by location demand. |
| Paid social (before/after, injectables) | Skip. You have no proof gallery yet, so it burns cash. | Test. Start small with real before-and-after content. | Fund now. Scale what the tests prove. |
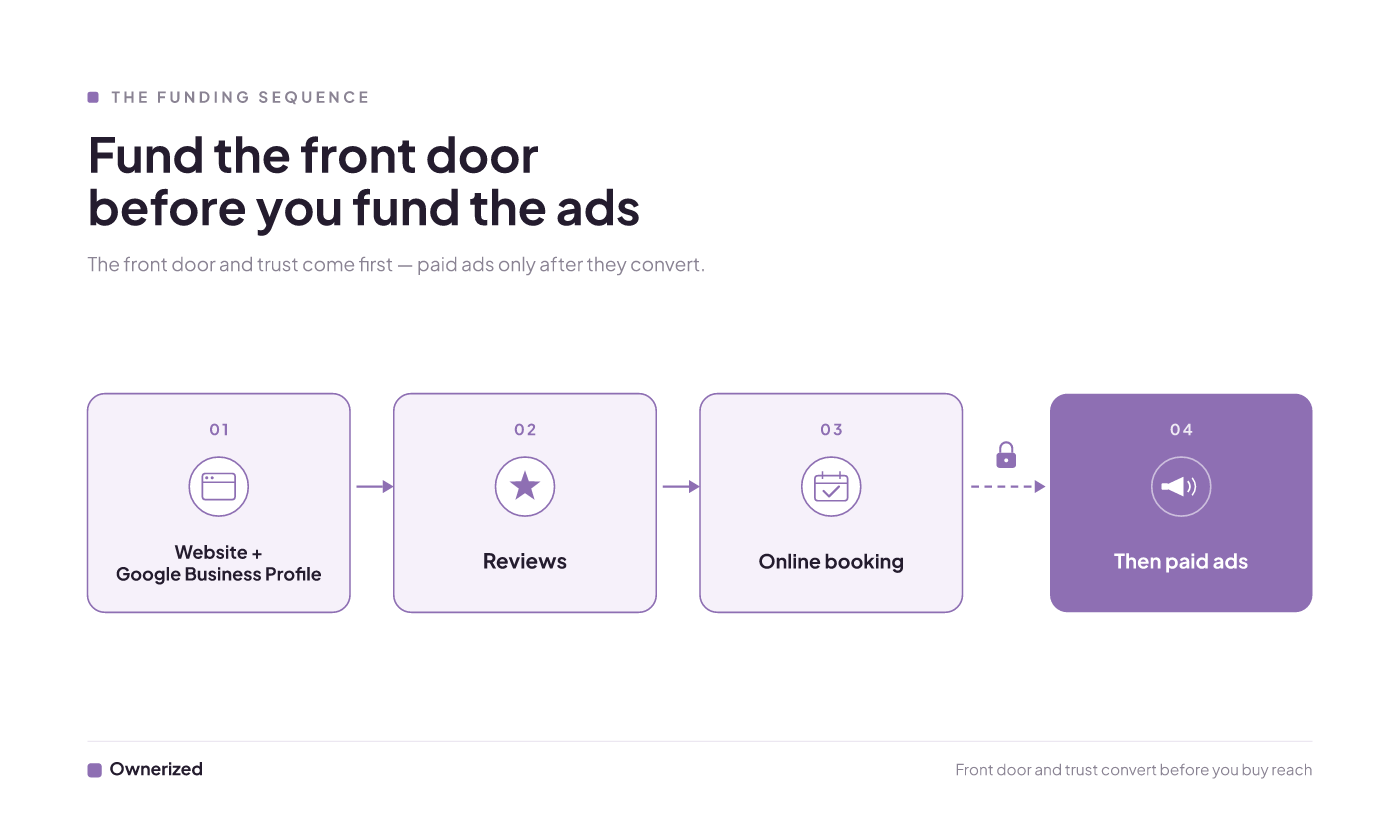
The funding sequence, in one line per stage:
- Brand-new: website and Google Business Profile, then reviews, then online booking. Paid comes only after those convert.
- Established: keep owned and earned sharp, add Google Ads on high-intent terms, then test paid social.
- Multi-location: standardize owned and earned across sites, then scale paid where demand is already proven.
One honest caveat. This ordering is reasoned from how the channels work and how aesthetics patients decide, not from a benchmarked cost model. No trustworthy cost-per-patient dataset for aesthetics clinics exists to lock it down. So treat the sequence as a strong default, then validate it against your own booked-appointment tracking.
What acquisition actually costs, and how to track your cost-per-patient
Acquisition costs materially more than keeping a patient you already have, and no one publishes a verified cost-per-patient figure by channel for cash-pay clinics. Anyone who quotes you a precise number for aesthetics is guessing. So the only figure that means anything is your own.
The formula is plain. Take your total marketing and sales spend, then divide it by the number of new patients it brought in. Run it over a rolling year, not a single month, so a slow February or a busy December doesn't distort the picture.
Run a quick illustration. If you spent $48,000 CAD across a year on ads, tools, and staff time, and it booked 320 new patients, your cost per patient works out to $150. Those inputs are made up to show the math, not a benchmark to copy. Now run the same calculation per channel. That is how you find out whether Google Ads is cheaper than paid social for you, at your clinic, in your city.
Measure booked appointments, not leads
A lead is a maybe. A booked, showed-up appointment is money. When you judge a channel by leads or clicks, you reward the channel that produces the most noise, not the most patients. Judge every channel by what it actually drives into your calendar.
That takes connected tooling. When your booking, marketing, and reporting talk to each other, each dollar of spend maps to real booked visits and nothing slips between the cracks. Two honest limits come with it. Connecting the tools takes setup work, and no attribution is ever clean, because a patient often sees an ad, reads a review, and asks a friend before they book. So give each channel a full booking cycle before you judge it, and watch the trend across quarters instead of reacting to one slow week.
Where new clinics waste acquisition budget
The fastest way to burn a small budget is to fund the right channel at the wrong time. Two traps catch new clinics again and again.
First, broad Google Ads before the site and profile convert. If you pay for clicks that land on a slow site or a thin profile, you are renting traffic that leaks straight back out. Fix the front door first, then buy traffic for it.
Second, chasing referrals before you have anyone to refer you. Referrals belong in every clinic's growth plan, but the system rewards a happy patient base. With no base yet, you are building a machine with no fuel. Put that energy into reviews and booking instead. Both traps are stage-bound, not permanent. The same Ads spend that wastes money for a week-one clinic can be an established clinic's best channel, so treat these as calls for your situation, not absolute rules.
Your next move, by clinic stage
Patient acquisition is a campaign to make a prospect choose you, so point every dollar at the step in front of you.
If you're brand-new, don't touch paid yet. Finish your Google Business Profile, publish a handful of real result photos with consent, and get frictionless online booking live so a prospect can convert without a phone call. Self-scheduling removes the phone-call barrier that quietly drops bookings.
If you're established, your owned and earned base already works, so layer Google Ads on high-intent local searches and test a small paid-social budget with your best before-and-after content. It's also worth checking how you show up when patients ask an AI assistant which clinic to choose, since answer-engine visibility is fast becoming its own front door.
If you're multi-location, standardize the basics, then scale paid where demand is proven and connect scheduling across every site so no location loses a booking to a broken handoff.
One last thing, true at every stage. No channel plan fixes a poor in-clinic experience or a booking flow that drops patients halfway. Fix the front door, then scale the spend. If you want a place to start, Ownerized maps every pre-booking signal a patient checks before they choose you.
Patient acquisition software: a Canadian med spa guide
By the end, a clinic owner can decide whether to buy patient acquisition software now, which category fits their stage, and the two conditions (retention performance and connected data) that determine whether any tool pays off.
Read insight
Healthcare marketing patient acquisition, ranked by payback
You will leave knowing what patient acquisition is, and a way to rank your channels by CAC payback instead of a to-do list of tactics — scoped to a Canadian med spa's economics.
Read insight
Med spa lead generation: what to fund first in Canada
By the end, a clinic owner knows the one channel to start with for their stage and budget, what to expect a booked patient to cost, which ad tactics will get rejected before they waste money, and how to convert the leads they get.
Read insight