Key takeaways
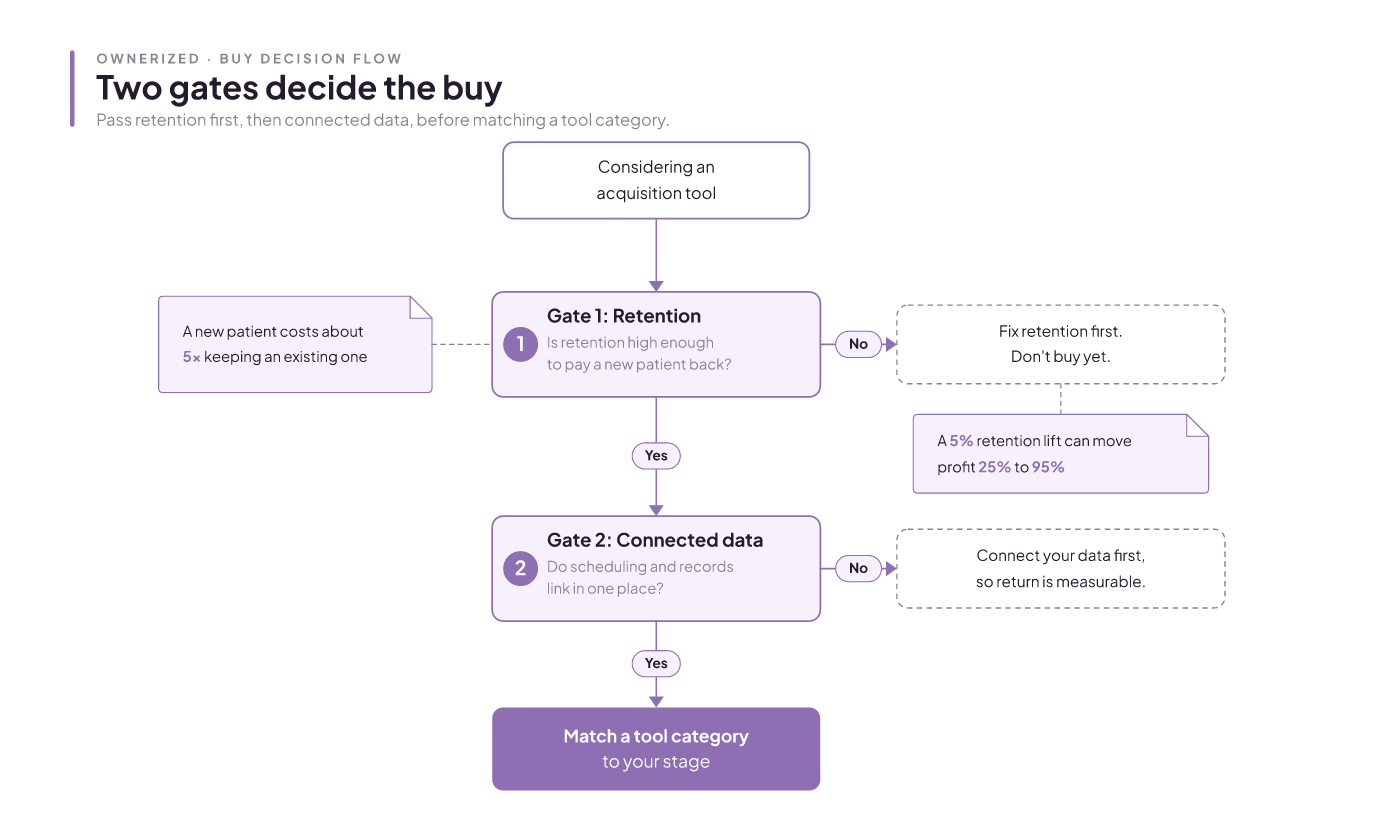
- Patient acquisition software wins new patients, but only past two gates.
- Retention gate: a new patient costs about 5x an existing one.
- A 5% retention lift can move profit 25% to 95%.
- Data gate: scheduling and records must connect before any tool pays.
You searched for a clear pick and got vendor pages and roundups where every shortlist opens with the publisher's own product. None of them tells a clinic your size which tool, and when. This guide does the opposite. It hands you a framework to decide which category fits your stage, and it gates the buy on two things the roundups skip. It names the category and the timing. It does not crown a single best brand, because the right answer depends on your retention and your data, not on a ranking.
What patient acquisition software actually is
There is no single clean product category called "patient acquisition software." It is a bundle of overlapping tools, and that overlap is a big reason the buying decision feels murky. You are not choosing one thing; you are choosing which of several overlapping jobs you actually need, which is exactly why the "best software" lists never land for a specific clinic. Here is the honest limit to sit with before you shop: because the category is this blended, no roundup can hand you one correct product, and this guide will not either. The most any framework can do is map the lanes and tell you which one your clinic needs first. Treat any list that opens with a single "best" pick as a marketing artifact, not a decision.
Patient acquisition itself is simple to define: it is the work of attracting, converting, and onboarding new patients. The software is whatever helps you do that without dropping people between the ad and the appointment.
It helps to separate three jobs that get lumped together:
- A CRM manages the relationship and the outreach: who a patient is, what they booked, when to follow up.
- An EHR holds the clinical record.
- A booking system runs the calendar, cuts no-shows with automated reminders, captures consent, and produces the operational data you need to grow.
The acquisition and intake layer that sits on top splits into four lanes: conversational intake that chats a lead through booking, intake modules bundled inside an EHR, dedicated form-and-check-in platforms, and general form builders adapted for healthcare. A healthcare CRM sits alongside these, securely holding patient information and automating outreach. Knowing which lane a tool lives in tells you what it will and won't do before you sit through a demo.
Why your retention caps the payoff
Here is the part the roundups leave out. Acquisition and retention are two sides of the same coin, and you cannot judge an acquisition tool without looking at retention first. The reason is cost. Bringing in a new patient runs about five times the cost of keeping one you already have. Push retention up by just 5% and profit can climb anywhere from 25% to 95%.
Run those two numbers together and the gate appears. If patients arrive and then drift away, an acquisition tool just fills a leaking bucket faster. You pay the 5x cost again and again to replace people you could have kept. Multi-clinic research has looked at how structured follow-up relates to retention, so this is not a hunch. Below a retention line you have to find on your own books, more acquisition spend loses money. Fix the leak first, and the same tool starts paying back.
The 5x figure and the 25% to 95% range are industry ranges, not your clinic's measured numbers. Treat the break-even as a rule to run on your own data, not a promise.
The retention math to run before you buy
You can calculate retention with one formula:
Retention rate = [(E - N) / S] x 100
E is the patients you have at the end of a period. N is the new ones you acquired during it. S is the count you started with. Strip out the new patients so you are measuring who stayed, not who arrived.
A worked example: start a period with 10 patients, end with 7 of them still active, and your retention rate is 70%.
One blended number hides a lot, so read retention over a window that matches how your clinic actually works, like a treatment recall cycle. A young clinic hits a wall here. The sample is too small to trust yet, so the percentage bounces around on a handful of patients. If that is you, measure anyway, but treat the number as a direction, not a verdict. You can walk through the full method in our guide on how to measure your clinic's retention rate.
The data floor: what must connect first
The second gate is quieter and easier to skip. Measuring retention, and measuring whether an acquisition tool earned its cost, both assume your data is connected. Scheduling and patient records have to talk to each other and be readable in one place. Without that, you buy a tool and then cannot attribute a single booking to it. You will feel busier and have no idea if you are richer.
So make this a pre-purchase checklist item, not an afterthought: can you see, in one place, where a patient came from and whether they rebooked? A booking system that reduces no-shows and captures consent is often where that connected data starts.
The honest catch: getting to a connected data floor can cost more time and money than the acquisition tool itself. Say it out loud in your planning, because it is usually the better first spend. A tool that measures return is worth more than a flashier one you can never grade.
Why generic tools miss a Canadian aesthetics clinic
General patient acquisition and retention software is sold to organizations of every size, from a solo practice to a hospital network. That one-size framing is exactly the problem. It is built for acute, one-off visits, and an aesthetics clinic does not run that way. Three workflows expose the gap:
- Injectable recall cadence. Your neuromodulator and filler patients come back on a rhythm, not once. A tool built for urgent care has no concept of a recall clock.
- Membership billing. Recurring memberships and package plans need billing and tracking that hospital and dental tools rarely handle.
- Before and after consent capture. Aesthetics runs on photo documentation tied to consent. Generic intake tools treat this as an edge case.
To be clear about the limit: this is an argument about fit criteria, not a tested verdict on named products. No first-party head-to-head of specific tools against an aesthetics workflow is offered here. What you get is a sharper set of questions to bring to any vendor. Software built for the aesthetics workflow, rather than adapted to it, starts from a different place.
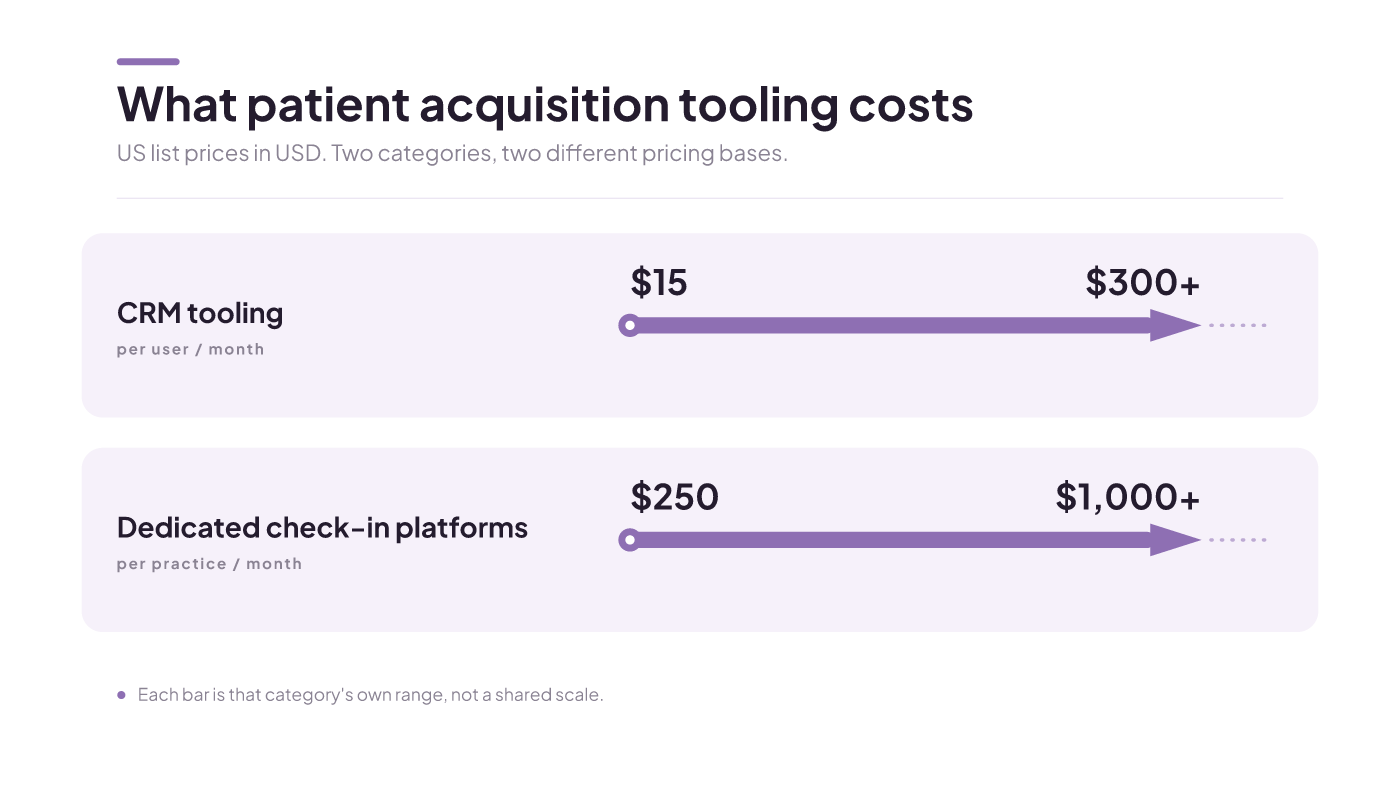
What it costs, and the pricing traps
Prices below are US list prices in US dollars. Canadian quotes come in CAD, carry different taxes, and will not match line for line, so use these to size a category, not to set your budget.
CRM tooling runs from about $15 per user per month to over $300 per user per month. That spread is wide even between tools that do similar things, which tells you the label on the box means little. Dedicated check-in and engagement platforms price differently, often starting near $250 per month and scaling past $1,000 per month per practice. The broader CRM market reached $73.4 billion in 2024 and is projected to pass $100 billion by 2027, so the tooling is not going away and the sales pressure will not either.
Two traps hide in these numbers. Per-user pricing looks cheap until every front-desk and injector seat adds up. And a low sticker often skips the integration work that makes the data floor real. One more figure worth holding: roughly 30% of patients abandon long digital intake forms before finishing, and clinicians lose about two hours to admin for every hour of patient care. A tool that does not cut that is a cost, not a fix.
Evaluation criteria and a decision table by stage
Score any tool against the same criteria, so you compare fairly instead of falling for the best demo. For a med spa, the core list is:
- Privacy-compliant charting with access controls and audit trails. Canadian clinics answer to PIPEDA and provincial health-privacy law, such as Ontario's PHIPA, not the US HIPAA regime most of these tools are built around, so confirm a vendor can actually meet Canadian rules.
- Before and after photo management with secure storage and patient consent.
- E-signature digital consent forms.
- E-prescribe, if your scope needs it.
- A patient portal.
- Integration with practice management, so booking and records do not force double data entry.
Then match your stage to a category. The gates decide more than the feature list does.
| Clinic stage | Retention gate | Data floor | Focus first | Category to consider |
|---|---|---|---|---|
| New, under about a year | Sample too small to trust | Often not connected | Connect scheduling and records, start measuring | Booking and practice management, not an acquisition tool yet |
| Growing, steady recall | Measure over a recall window | Getting there | Fix retention leaks | CRM or recall, plus booking integration |
| Established, strong retention | Passed, verified on your books | Connected and measurable | Filling open capacity | Dedicated intake or check-in, or a CRM with acquisition |
A table cannot capture your exact stack or contract terms. Integration depth in particular only proves itself in a demo run against your own data, not on a feature sheet. Independent software directories keep a dedicated medical-spa software category built on verified user reviews, which is a fair place to start a shortlist before you book demos. For tools scoped to the aesthetics workflow, our roundup of aesthetician software goes deeper on the category.
Demo questions that expose a bad fit
A demo is built to show strength. These four questions surface the weakness instead, and each maps to one of the evaluation criteria above and to one of the four intake lanes a tool can live in:
- Show me a recall sequence for a filler patient at three, six, and nine months. Watch whether recall is native or bolted on. This is the injectable recall cadence, and a tool built for one-off acute visits has no lane for it.
- Bill a membership and a single treatment on the same account. Recurring membership billing is where generic intake tools crack, because hospital and dental systems rarely handle package plans.
- Take a before photo, attach consent, and pull both up nine months later. This tests before and after photo management with secure storage and patient consent, the aesthetics core that adapted tools fumble because they treat photo-plus-consent as an edge case.
- Where does this pull my booking data from, and can I see patient source on one screen without double data entry? If they cannot answer, the connected-data floor is not there, and you will not be able to attribute a single booking to the tool.
Each question is a gate, not a preference: fail the recall, billing, consent, or data question and the tool is a category mismatch, not a close call. If a vendor cannot do these live, the mismatch is real, whatever the ranking said.
Common objections, answered
"Just buy the all-in-one and be done." An all-in-one only pays off once your data is connected and your retention holds. Bolt acquisition onto a leaking clinic and you scale the leak. The rule: gates before features.
"We are new, so retention does not matter yet." It matters most now, because you cannot compute payback without a retention history. A new clinic with no recall data yet cannot tell if an acquisition tool earns out. Start on the data floor, not the tool.
There is a real case for buying acquisition tooling early. If your retention is already strong, your scheduling and records are connected, and you have open capacity to fill, you have cleared both gates and the math works in your favour. The advice is not "always wait." It is "clear the gates first," and some clinics already have.
What to do next, by where you are
Sequence beats speed here. The fastest path to more patients is usually fixing retention and data before you buy anything.
- If you are new: connect scheduling and records, then start measuring retention. Skip acquisition tools for now.
- If you are growing: calculate your retention rate with the formula above over one recall cycle, then plug the leaks before you add acquisition spend.
- If you are established with strong retention and connected data: match a tool category to your stage and book demos with the four questions in hand.
The honest version of this advice delays a purchase you may be eager to make. That is the point. Start by measuring your retention rate, then decide which patient acquisition strategies to fund first. The tool comes after the gates, not before.

Healthcare marketing patient acquisition, ranked by payback
You will leave knowing what patient acquisition is, and a way to rank your channels by CAC payback instead of a to-do list of tactics — scoped to a Canadian med spa's economics.
Read insight
Med spa lead generation: what to fund first in Canada
By the end, a clinic owner knows the one channel to start with for their stage and budget, what to expect a booked patient to cost, which ad tactics will get rejected before they waste money, and how to convert the leads they get.
Read insight
Patient acquisition strategies for Canadian aesthetics clinics: what to fund first
By the end, a Canadian aesthetics operator has a channel-by-clinic-stage-and-budget funding sequence they can keep, knows which channels to skip when starting out, and understands how to track cost-per-patient honestly instead of chasing le
Read insight