Key takeaways
- Patient retention rate = (patients at the end - new patients) / patients at the start x 100.
- Measure it per treatment cohort and time window, not one blended clinic number.
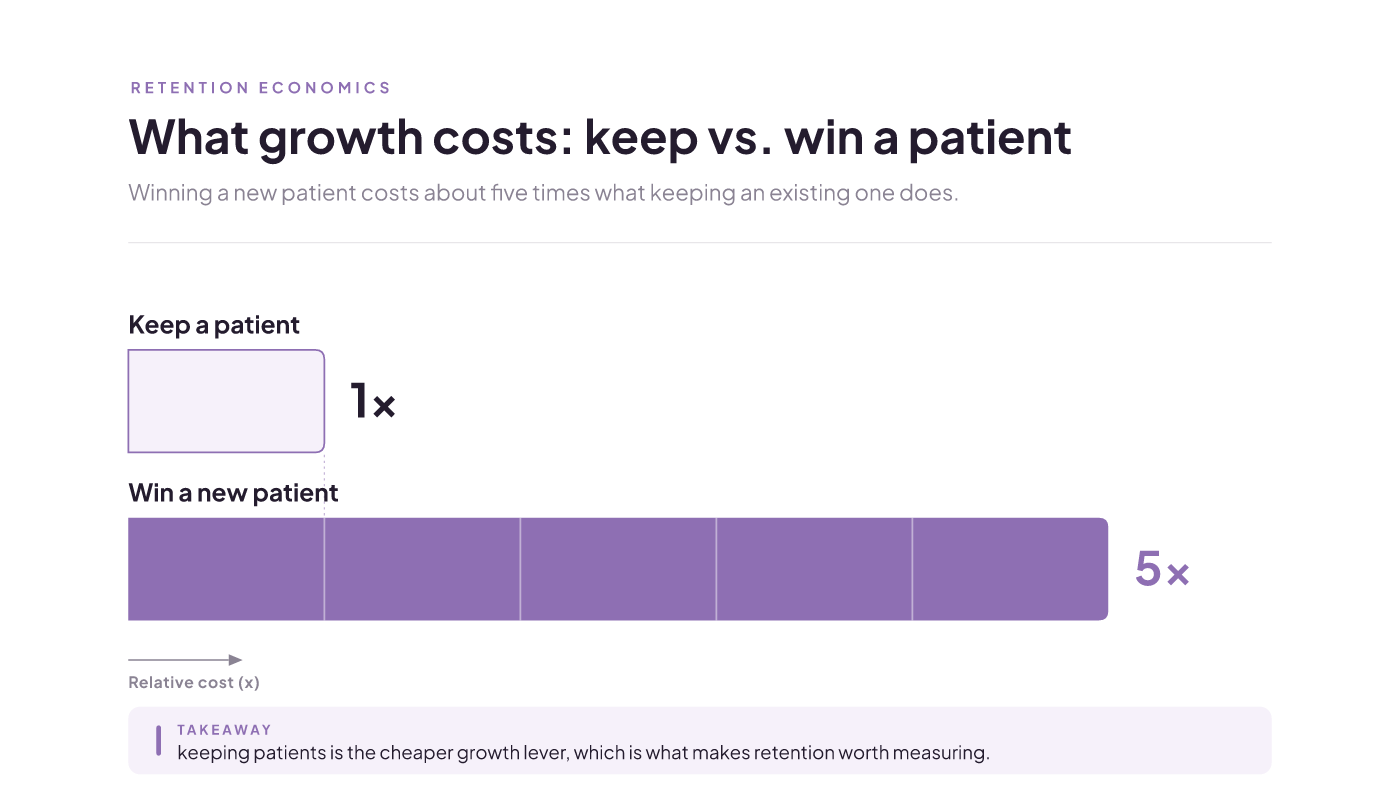
- Retaining a patient costs about a fifth of what winning a new one does.
- No universal "good" rate exists for aesthetics. Watch your own trend instead.
You can find the retention formula in one search. What you can't find is how to measure patient retention rate in a way your aesthetics clinic can actually act on: which patients to count, over what window, and whether your number is any good. That gap is the real work, and it's what this guide walks through.
What patient retention actually measures
Patient retention is the share of your existing patients who come back for care within a period you choose. Some people call it patient loyalty or the repeat-visit rate. It's the same idea under different names.
The retention rate turns that into one number from three counts: patients at the start of the window (S), patients at the end (E), and new patients you gained during it (N).
Watch the word "retention," because it travels across industries and the meaning shifts. Employee retention rate tracks which staff stay on payroll. Customer or SaaS retention rate tracks paying accounts that renew. This page uses the clinic sense: a patient who returns. So your number isn't comparable to an employee retention rate or a software churn figure, even when the math looks identical.
What you need before you can measure it
Before any arithmetic, you need three clean counts out of your practice management software (PMS) or EMR. Measuring retention assumes that scheduling and patient-record infrastructure is already in place, which for a modern aesthetic practice it usually is.
Pull these for your chosen window:
- Active patients at the start (S).
- Active patients at the end (E).
- New patients acquired during the window (N).
The catch is N. Your system has to tag new patients apart from returning ones for the whole window. If it can't do that cleanly, N becomes an estimate, and your rate is directional rather than exact. That's fine to start with, as long as you know it. If your PMS can't produce these counts without hand-sorting, fix the tagging first, then measure.
The formula, worked with real numbers
The standard patient retention rate formula is [(E - N) / S] x 100. It's the same equation healthcare and dental practices use, which is also why you'll see it written as the customer retention rate formula. The context changes; the math doesn't.
Here's how to calculate retention rate with real numbers. Say you start the window with 10 patients. By the end, 7 of them have come back, and none of those 7 are new. Divide 7 by 10 and multiply by 100, and your retention rate is 70%.
Two things about that number. First, you subtract N so fresh acquisition doesn't quietly inflate the rate. The formula counts patients at the end minus the new ones you gained, so a clinic can grow its total for the period and still be quietly losing the base it started with. Second, this single blended figure is where you begin, not where you stop. It averages every treatment line together, so it can look healthy while one service is churning underneath.
Measuring patient retention by cohort and window
One blended clinic-wide rate hides more than it shows. The stronger approach is to pick a timeframe and a cohort, look at their history, then watch that group going forward.
A cohort is just a group you define. In aesthetics, treatment lines are the natural cut. So instead of one number, you might track your injectables patients from the first quarter and ask how many rebook within your window. Then do the same for laser, for facials, for body work.
The blended rate might read 70%. Slice it, and you could find injectables higher and a newer laser line well below the average. Same clinic, very different stories. The blended average buried the one you needed to act on.
The trade is sample size. A single cohort is a smaller group, so its rate bounces around more month to month. You give up some precision on any one number to see where retention actually leaks. For deciding where to spend attention, that's a good trade.
Separate true retention from reactivation
The formula has one honest move built in: subtracting N. New patients don't count as retained, because they were never at risk of leaving yet. Take them out and the rate reflects the base you started with, not this period's marketing.
The harder call is the lapsed patient who resurfaces. Someone had filler 20 months ago, went quiet, and just rebooked. Retained, or new again? There's no universal cutoff. You have to set a lapse window, say 12 or 18 months, past which a returning patient counts as reactivated rather than continuously retained. Reasonable clinics pick different lines.
What matters more than the exact number is applying it the same way every period. Pick your lapse rule once, write it down, and don't move it. A rule you keep steady lets you compare periods honestly. A rule you change every quarter turns your trend into noise.
What counts as a good rate, and what 80% means
Start with what the number literally says. An 80% retention rate means 8 of every 10 patients from your starting cohort returned inside your window. Nothing more mystical than that.
Now the question everyone asks: what is a good patient retention rate for an aesthetics clinic? The honest answer is that no defensible aesthetics-specific benchmark exists. Numbers borrowed from dental, physiotherapy, or SaaS aren't your business, and treatment mix and lapse windows differ too much between clinics for a single target to mean much.
So judge your number against yourself. Hold the cohort definition and window steady, then watch the direction across periods. A rate that climbs on the same definition beats hitting some percentage you read on a competitor's blog. Your own trend is the benchmark that's actually yours.
Why the number is worth tracking
The effort pays off because of retention economics. Winning a new patient can cost roughly five times what keeping an existing one does. And a 5% lift in retention can move profits by 25% to 95%. Those figures come from broad customer-retention research rather than aesthetics studies, so read them as the direction of the effect, not a promised number for your clinic. The direction is what makes the metric worth watching.
There's a clinical driver too. A peer-reviewed, multi-clinic real-world analysis links formal, structured facial assessment and treatment planning to higher patient retention in aesthetic practice. The published work doesn't give a clean effect size you can bank on, so treat it as a real association, not a guaranteed lift. The takeaway holds anyway: how you assess and plan a patient's care is part of whether they come back, which means retention is something you can influence, not just observe. To see where a retained-patient dollar sits against acquisition spend, the economics are worth mapping against your own book.
Where the numbers go wrong when you pull them
Most bad retention rates come from bad inputs, not bad math. Two failures show up again and again.
The first is a polluted S. If your starting base sweeps in one-visit consult no-shows or enquiries that never converted, you've padded the denominator with people who were never really patients. The rate sinks for a reason that has nothing to do with loyalty. Decide what an "active patient" means for you, and count only those in S.
The second is leaving your window undefined. A retention rate always sits on top of a look-back period, and the only question is whether you picked it. If you don't set one, your export uses whatever period it falls back to, and the rate shifts between quarters for a reason you can't trace. There's no single correct definition of "active patient," and exports differ by system, so the fix isn't hunting for the one right setting. Decide your inclusion rule and your window once, write them down, and apply the identical ones every period.
How to know it worked, and what to do next
You'll know you measured retention correctly when the number is repeatable. Track the same cohort under the same rules across two consecutive windows and watch the direction. A comparable series is the proof; a one-off percentage isn't.
Remember that retention lags treatment. A patient you see today might not rebook for months, so a single window is a snapshot, not a trend. You need at least two comparable periods before the number can tell you whether a change, like tightening your assessment and planning, is actually working.
So your next step is small and concrete. Pick one treatment cohort, pull S, E, and N for a clear window, and compute that cohort's rate. Then do it again next period with the exact same rules. Two clean, comparable numbers beat one blended rate you can't trust. From there, the same discipline you use to bring patients in is what keeps them coming back.
Patient acquisition software: a Canadian med spa guide
By the end, a clinic owner can decide whether to buy patient acquisition software now, which category fits their stage, and the two conditions (retention performance and connected data) that determine whether any tool pays off.
Read insight
Answer engine optimization (AEO): a guide for clinics
By the end you'll know what AEO really is, why the training-data mental model most guides use is wrong, which answer surface to prioritize for a local Canadian business, and which tactics are worth your time versus which are unproven.
Read insight
Healthcare marketing patient acquisition, ranked by payback
You will leave knowing what patient acquisition is, and a way to rank your channels by CAC payback instead of a to-do list of tactics — scoped to a Canadian med spa's economics.
Read insight