Key takeaways
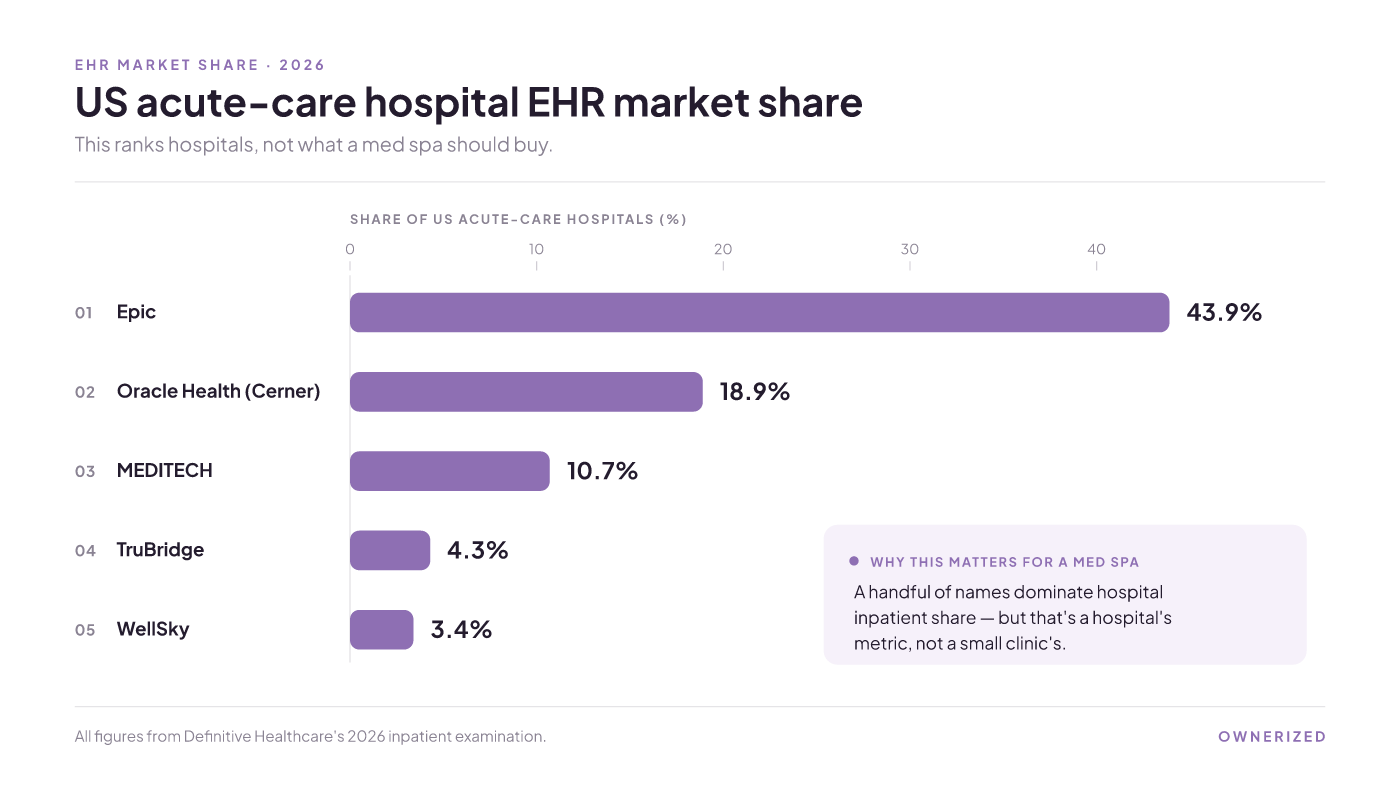
The famous names, Epic, Oracle Cerner, and MEDITECH, top every EHR list because they rank US hospital share. Epic leads US acute-care hospitals near 44%. But none of them is built to hold a med spa's record, so pick on capabilities, not fame.
The names that top every list of EHR systems
Search "list of ehr systems" and you get the same roster every time: Epic, Oracle Health (the former Cerner), and MEDITECH. These are the names of medical EHR systems that show up on almost every roundup, and for good reason. The market is huge and crowded. More than 500 vendors sell some form of EHR product, yet a small group controls most of the subscribers and revenue.
So what are the top 5 EHR systems by the number most lists use? In US acute-care hospitals, Epic holds about 43.9% of the market, Oracle Health/Cerner about 18.9%, MEDITECH about 10.7%, TruBridge about 4.3%, and WellSky about 3.4%, per Definitive Healthcare's 2026 inpatient examination. That is your "top 3 EHR systems" and your "largest EHR systems" answer in one line: Epic, then Oracle Cerner, then MEDITECH.
The market keeps growing too. The global EHR market sits around $35 billion and is expanding at roughly 15.1% a year. The US acute-care slice alone was worth about $26.4 billion in 2024.
Here is the catch. Every one of those figures measures hospital inpatient systems. It answers a 400-bed hospital's question, not a two-provider clinic's. The most popular EHR system in a hospital is popular because it runs a hospital: many departments, thousands of beds, records shared across a whole network. A single-location aesthetic clinic in Canada shares almost none of that. So the ranking is real, but it is the wrong yardstick for your buy.
EMR vs EHR, and why the difference flips for a one-location clinic
You will keep hitting the EMR-versus-EHR distinction, so here is the plain version. An EMR is the digital version of a paper chart for a single practice. It holds a patient's history, diagnoses, medications, and test results inside that practice's own system, and clinics have worked this way for decades. An EHR is the broader idea: a record built to be shared across providers and organizations, so a hospital, a lab, and a specialist can all read the same file.
Most lists treat "more shareable is better." For a hospital, it is. For a standalone med spa, that advice flips. If you run one location with one to three providers, cross-provider interoperability barely touches your day. You are not handing charts to a referring hospital. What decides your buy instead is whether the system books appointments and takes payment natively, in one place. That is the work your front desk does every hour.
One honest caveat. If you plan to refer patients into or out of a hospital network, or add multiple sites later, interoperability starts to matter again. This inversion holds for a genuinely single-location practice, not for every clinic.
What the generic lists leave out for a med spa
Take Epic, Cerner, or MEDITECH and try to run a cosmetic treatment through them. The record a med spa lives on is not there. Four charting jobs decide whether a system fits an aesthetic clinic, and the hospital-grade names are not built for any of them out of the box.
- Structured treatment charting. Customizable SOAP notes and treatment protocol templates, so each session's plan, products, and notes drop into a repeatable format instead of a free-text box.
- Before-and-after photo series with consent. Photos are your clinical proof and your marketing, and they have to sit against the visit with the signed release stored beside them.
- Digital cosmetic consent with e-signatures. Every treatment needs a consent captured, dated, and findable.
- Native booking and point of sale. Scheduling and payment built into the record, not bolted on, so the front desk is not double-keying between a booking app and the chart.
Under all four sit the basics you still need: charting with encryption, access controls, and audit trails, plus a patient portal and e-prescribing where your treatments call for it. Records also have to meet Canadian privacy law, which is a floor, not a feature.
Skip these and the cost is not the monthly fee. It is fragmentation. Start with a booking app, then bolt on a separate EMR once you add injectables or laser, and you end up with client photos in one tool, consent forms in a second, and clinical notes in a third. The real bill is the staff hours spent reconciling records across those tools, and the compliance gap when a consent form or a product lot number is not where an auditor expects it.
Two ways a med spa buys the wrong system
There are only two common mistakes, and they pull in opposite directions.
The first is overbuying. You take the "safest" name off the top-10 list, a hospital-grade EHR built to run a 400-bed hospital across many departments, and pay for interoperability and inpatient depth you will never use, while it still is not built to hold a before-and-after photo series or run your front-desk booking. The second is underbuying. You start with a sleek booking app because it is cheap and easy, then scatter your clinical record across three tools the moment treatments get regulated: photos in one, consent forms in a second, notes in a third. The real cost of that split is the staff time spent reconciling records across the tools, and the compliance gap when a consent form or product lot number is not where an auditor expects it. One overpays for the wrong strengths. The other underpays and inherits that reconciliation and audit risk. The fix for both is the same: start from the four charting jobs, not from a market-share table.
Match the system to your practice type
The right category depends on what your practice actually is. This table maps practice type to the capabilities that matter and the kind of system that fits. It is built from public capability descriptions and the checklist above, not a hands-on teardown, so treat it as a pointer to the right shortlist, not a verdict on one winner.
| Practice type | Must-have capabilities | Entry price tier | Native booking | Don't choose this if |
|---|---|---|---|---|
| Single-location clinical med spa | Treatment templates, photo series, e-consent, native booking | Low to mid monthly | Yes | You need multi-hospital record sharing |
| Multi-location salon and spa group | High-volume scheduling across sites, central reporting, POS | Mid to high | Yes | You are one room and want deep medical charting, not scale |
| Booking-first, light-charting practice | Clean client experience, deposits, simple notes | Low monthly | Yes | Your treatments need real clinical charts and consent trails |
| Hospital-affiliated or multi-site clinical | Cross-provider interoperability, deep EMR, e-prescribe | High | Varies | You are a standalone clinic that never refers out |
Read across a row, then be honest about the "don't choose this if" cell. That column is where most buyers go wrong, because they shop for a category that flatters their ambitions instead of one that matches their week.
The short list a Canadian small clinic actually lands on
The hospital directories will not tell you what a Canadian clinic buys, so here it is in plain terms. Three general systems come up constantly north of the border. Jane App is a mainstay in allied-health and clinic settings, and widely cited figures put it near a 4.8 rating across thousands of reviews. TELUS Health runs several EMR products used by a large share of Canadian physicians, with commonly cited numbers above 40,000 doctors nationwide. OSCAR is a free, open-source EMR that suits practices with in-house technical support to run it.
None of these is aesthetic-specific out of the box, which is the honest limit. They are strong general records, not cosmetic-charting tools with treatment templates and native point of sale baked in. To build a neutral starting list, independent directories such as Capterra.ca keep verified user reviews across medical-spa software and list every provider, not just the ones that pay them. Use one to gather candidates, but remember it also carries sponsored profiles, so it builds your shortlist rather than picking your winner.
What these systems actually cost in year one
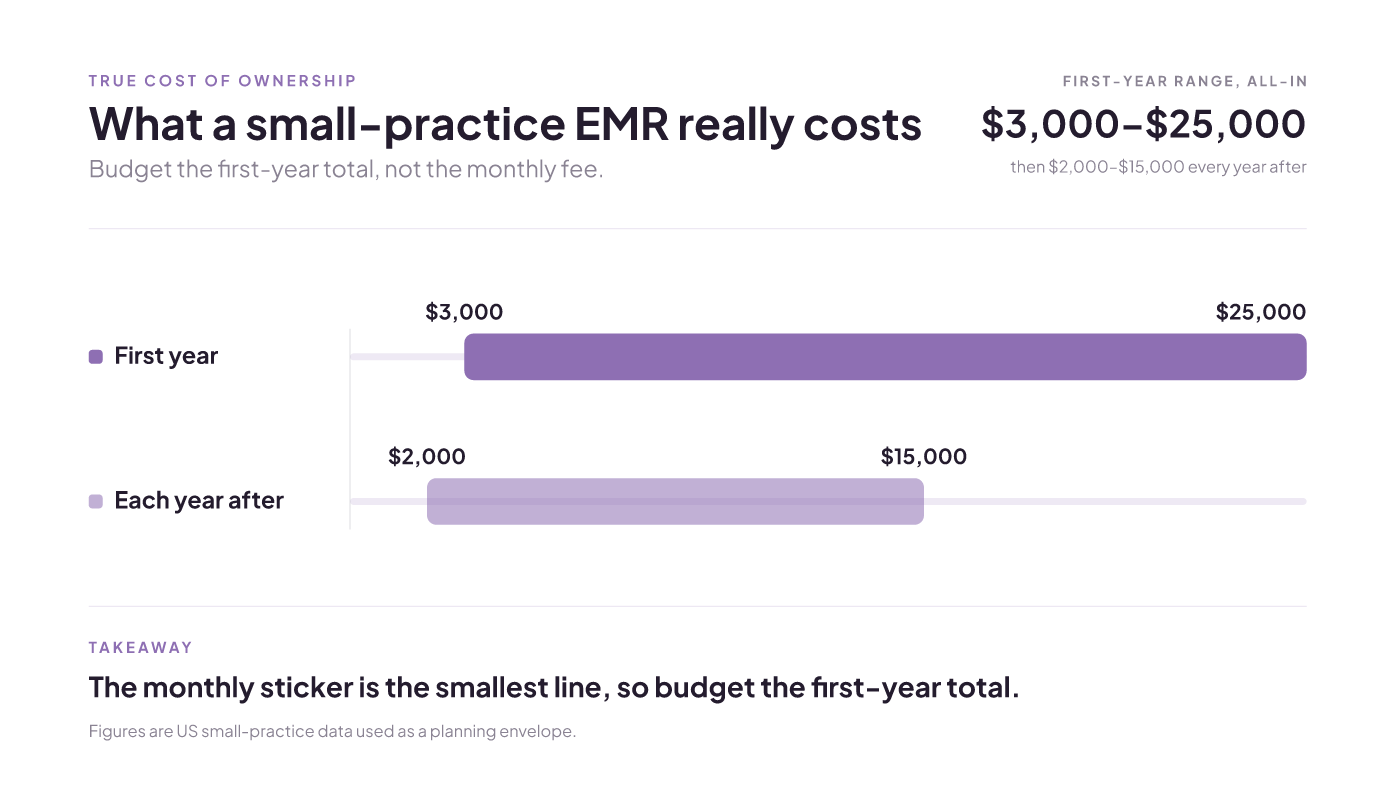
Sticker price lies, because the monthly fee is the smallest line. Published small-practice figures put EMR software at roughly $3,000 to $25,000 in the first year, and $2,000 to $15,000 per year after that, once you count implementation, data migration, training time, interfaces, and optional modules like billing, ePrescribing, and patient texting.
Those ranges come from US small-practice data, so use them as a planning envelope and confirm current Canadian pricing in your own dollars before you commit. Aesthetic-capable tools do publish low entry tiers, some at a modest monthly rate and others priced higher for deeper EMR features. Entry prices move often, so verify the current number with the vendor rather than trusting a figure you saw on a list. Budget for the first-year total, not the headline monthly fee, and the comparison between systems gets a lot more honest.
How to build and pressure-test your own shortlist
With over 500 vendors in the market, no single list is complete, including this one. So the durable skill is a method you can rerun, not a name to memorize. Four steps:
- Start from a neutral directory such as Capterra.ca and pull a handful of candidates that actually serve aesthetic clinics.
- Score each one pass or fail on the four charting jobs: structured treatment templates, before-and-after photo series with consent, e-signature cosmetic consent, and native booking with point of sale.
- Confirm the system is available and supported in Canada, and that it meets your provincial privacy rules.
- Compare true first-year cost, not monthly price, across the survivors.
This guide synthesizes public sources and a capability framework, not a hands-on scorecard we ran ourselves. So treat the shortlist as your starting five, then book demos and run each finalist against your own workflows before you sign. If booking and deposits are your first pain, our independent Canada ranking of medical spa booking software turns this shortlist into systems you can book demos against, and our guide to scheduling software for a Canadian medical office is the place to start if scheduling is the whole job.
Aesthetician software in Canada: booking app or EMR?
By the end, the reader can classify any aesthetician software into booking-first or full-EMR, run a 7-point checklist against their own clinic, and know which category they should be shopping in, and why the monthly price is the wrong thing
Read insight
Scheduling software for medical office: a Canadian guide
Leave knowing which 'best scheduling software' rankings are self-serving, what these tools actually cost per month, where the HIPAA/compliance tier trap sits, and which class of tool fits your office type, with Canadian privacy law kept str
Read insight
Medical spa booking software: an independent Canada ranking
An ownership-neutral, disclosed-rubric ranking of medical spa booking software that scores each tool on rebooking/retention across a multi-month journey and on Canadian PIPEDA/PHIPA fitness, and tells you which popular 'best of' guides are
Read insight